From her earliest days in school, 13-year-old Zara in Nepal struggled to get by. She couldn’t read what her teachers wrote on the blackboard, and she often rolled her eyes around and made unusual body movements, instantly making her stand out as “different” to her peers. We can only imagine how lonely and confusing life was for the girl – not knowing why she was so unlike the other children.
What nobody realized was that some of Zara’s actions – the eye-rolling, the strange movements – are typical self-stimulatory behaviours seen in some children with severe vision impairment. As a result of these behaviours, children like Zara are sometimes misdiagnosed with autism or developmental disabilities if their low vision continues to go unrecognized.

Fortunately for Zara, her school was included in a school eye screening project we had implemented in collaboration with our partner, Nepal Eye Hospital. During the screening, community health workers discovered that Zara had cataracts in both of her eyes, a condition she’d been born with, and that had severely clouded her vision throughout her young life.
The outreach team met with Zara and her mother, explained the condition to them, and told them that treatment was available. They referred the family to the nearby Simara Vision Centre for a thorough examination, where doctors confirmed the diagnosis of congenital cataracts. From there, Zara received a further referral to Nepal Eye Hospital in Kathmandu for surgery.
The Operation Eyesight project team provided crucial support, guiding Zara and her parents through the treatment process and helping them access surgery at a reduced cost, making it affordable for the family, who had limited financial resources.
Zara’s first eye surgery was a success, and a month later she returned to the hospital for surgery on the second eye. On her second visit, when she spotted Operation Eyesight’s Project Coordinator from across the hospital, she waved enthusiastically – something that would not have been possible before her first surgery.
Zara’s transformation was profound. The eye rolling stopped, her unusual movements decreased, and she became more sociable with family and friends, even interacting withstrangers. For the first time in her life, she could recognize people from a distance, read the blackboard in class and fully participate in school activities.
Zara’s mother was overwhelmed with relief to see her daughter blossom. She had been extremely worried about her child’s future, and was amazed to see Zara playing, learning and interacting like other children her age. She and her family expressed deep gratitude to the hospital, the doctors and healthcare workers, and to Operation Eyesight’s generous donors, for making this life-changing transformation possible.
Make a donation to help us reach more children like Zara with life-changing eye surgery.
Written with files from Anisha Gurung, Operation Eyesight’s Project Coordinator at Nepal Eye Hospital.
If you sprain an ankle or come down with a bad cough, your first stop is usually your family doctor. But when it comes to blurry vision, the path to care often looks very different. Around the world, eye health is still treated separately from primary health care, creating gaps that leave people without the vision help they need. Even in countries with universal health coverage, you might receive a complex eye surgery at no cost, yet pay out of pocket – or use private health insurance – for something as simple as a pair of eyeglasses.
At Operation Eyesight, we believe this needs to change. That’s why we’re working to strengthen areas of overlap between primary eye care and primary health care in our countries of operation. That means supporting the World Health Assembly’s integrated people-centred eye care (IPEC) resolution by working to integrate eye health into national health systems – and increasing access to free or subsidized eye health care.
It also means addressing the root causes of avoidable vision loss. In some regions in Africa, we bring fresh water and hygiene education to communities to help prevent infectious eye conditions. We also work to make sure our services offer more than just eye care, but can also link patients to other types of health care.
Health conditions rarely exist in silos – and vision loss is no exception. Diabetes, for example, increases the risk of eye conditions like cataracts. For 15-year-old Vanessa in Zambia, blurry vision was one of the first signs of the disease. When she started having problems reading the blackboard at school, a teacher sent her to our vision centre in her community of Matero for a checkup. From there, she received a referral to our partner hospital, where she learned that she not only had cataracts, but diabetes as well. Doctors helped her get her blood sugar levels under control, and then she got cataract surgery. Today, she is managing her diabetes and thriving in school, with dreams of becoming a doctor.

Vision problems can also cause a downward mental health spiral. Benson, a farmer in Kenya, lost his ability to work due to poor vision. As a result, he became angry and depressed, then turned to alcohol and drugs to cope with his situation. Luckily, his family got him into a drug and alcohol rehabilitation facility, where a visiting doctor diagnosed him with cataracts. Benson underwent surgery on both eyes, provided free of charge thanks to the support of our donors, and can see clearly now. Buoyed by his miraculous recovery, Benson finished up his time at the rehabilitation facility and happily threw himself back into farming.
In Canada, where Operation Eyesight is based, navigating eye care can be confusing. While the Canada Health Act covers medically-necessary eye health services, routine vision care like eye exams and prescription glasses often isn’t part of the deal. That leaves provinces and territories to fill in the gaps, and the result is a patchwork system. For example, seniors in Ontario get routine eye exams covered once they hit 65, but in Newfoundland and Labrador, those same seniors might have to pay out-of-pocket. It’s inconsistent, and it’s especially tough on vulnerable populations.
There is some support through the Federal Non-Insured Health Benefits (NIHB) program, which covers eye exams and eyewear for eligible First Nations and Inuit individuals. But even that has its hurdles: remote communities, limited healthcare infrastructure and cultural differences that make accessing care more complicated than it should be.
The passage of the National Strategy for Eye Care Act in 2024 was a major step forward in addressing these issues. As chair of the Canadian Eye Health Coalition, Operation Eyesight is helping shape a national framework that prioritizes equitable access to vision care. Our Global Director of International Programs, Kris Kelm, explains why it’s important that we have a seat at the table during the consultation period and beyond.
“We know that there will be many voices in this conversation with diverse interests, and we want to ensure there is representation from patients who have the least means and the least ability to access vision care,” he says. “The fact that we have over 60 years of experience working in this sector gives us a strong background to speak credibly to how we need to approach things in Canada, and our community partners can provide valuable insights to help shape eye care for all.”
He adds that Canada can learn from some of our countries of work, where eye health has been better integrated into the overall health systems and other public frameworks. As an example, he points to Ghana, where we work with the ministries of health and education to screen and treat students for eye conditions in the public school system. We have similar programs in Kenya and Zambia, too.
Another example is in India, where we are working with state governments to establish vision services in pre-existing government health centres. Building the capacity of vision care facilities within the country’s national health care system ensures that services reach the most underserved populations, as patients who are able to pay most typically seek care at for-profit facilities, rather than attending government services.
Shakuntala, in Madhya Pradesh, India, spends her days walking door to door through villages in her region, checking in on the health and well-being of families. She’s one of the million-strong network of Accredited Social Health Activists (ASHAs), employed by the Indian government, who deliver primary health care at the community level.
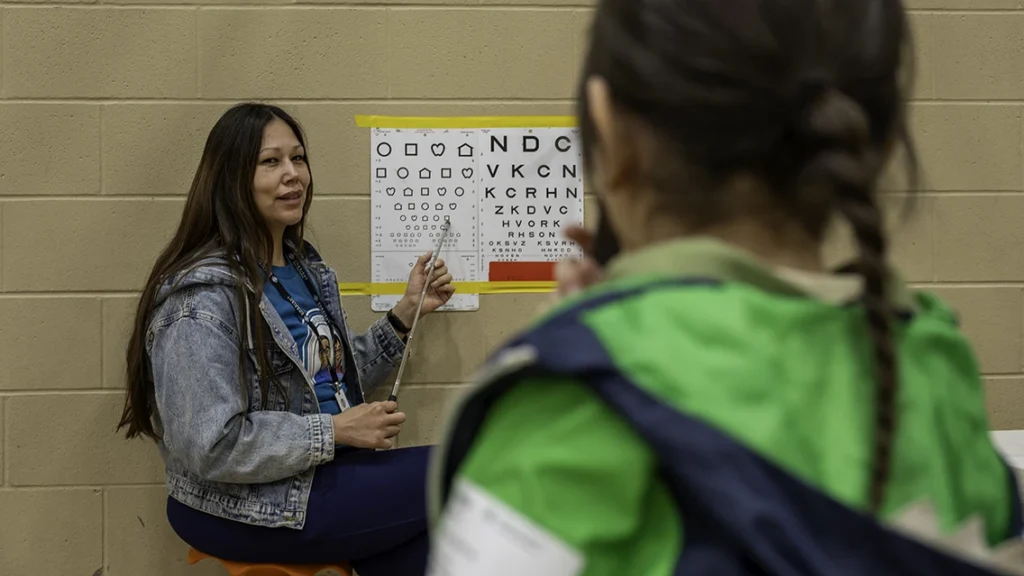
Her work includes providing pregnancy advice, supporting newborn care, educating parents about vaccinations and vitamins for children, and making all kinds of referrals to local clinics and hospitals. In 2022, Shakuntala added another set of skills to her toolkit: conducting primary eye health screenings, thanks to training provided by our Operation Eyesight team, in partnership with the Government of Madhya Pradesh. Shakuntala learned to measure visual acuity using an eye chart. She also learned to identify the signs and symptoms of various eye conditions. Once she identifies a patient with a possible eye condition, she refers them to the base hospital for diagnosis and treatment. In the meantime, she continues to provide advice and referrals on nutrition, vaccinations, prenatal care and other health concerns.
Shakuntala is just one of the thousands of community health workers we work with across the globe. In all our countries of work, we partner with existing health systems to recruit community health workers, mostly women, to help us deliver our programs. The health workers develop strong ties within the communities, resulting in high acceptance and trust in our programming.

Mabel, a community health nurse in Ghana, was trained in primary eye care so that she could identify eye health issues in addition to her regular duties. She says that being able to screen people at their home allows her to reach many women and girls who probably wouldn’t have left the village to seek eye health care, due to household responsibilities.
Anyone who has had a case of pink eye knows that having red, inflamed and itchy eyes isn’t much fun. But in some parts of the world, an eye infection can be a much more serious problem. Trachoma is an infectious eye disease that leads to vision loss and blindness in millions of people across the globe. It spreads easily through contact with eye discharge from infected people on hands and clothing, and through flies. If left untreated, chronic infections turn the eyelid inwards, causing intense pain and scarring of the cornea, which can lead to irreversible blindness.
Trachoma is preventable, and clean water is key to curbing the spread. When communities have access to clean water, people can clean their hands, faces and clothing more often, which prevents it from spreading.
In countries like Zambia, we work with Water Affairs (the government department responsible for water) to drill, rehabilitate and repair boreholes near where people live, work and go to school, so that whole villages have access to clean water. We also provide training to local volunteers in these communities in WASH (Water, Sanitation and Hygiene) and borehole repair and maintenance to ensure the clean water continues to flow. In areas where trachoma is endemic, we also work with partners to distribute antibiotics, which both treats and prevents trachoma.

It's another way that we work to address one of the root causes of avoidable vision loss, but it also helps us tie into improved health outcomes overall. Accessible clean water helps prevent dozens of infectious diseases. It also improves quality of life for women and girls, who are often tasked with the job of fetching water, which can take up hours out of the day and prevent them from participating in school, work or other activities. Moreover, clean water means people can grow vegetable gardens, raise livestock and keep entire families, and communities, happier and healthier.
When we invest in sight, we invest in education, productivity and dignity. To eliminate avoidable vision loss, vision care needs to be recognized as a public health priority and integrated into national health strategies. Operation Eyesight’s global experience – from rehabilitating boreholes in Zambia to collaborating with partners on new policies in Canada – demonstrates that integrating eye health into primary care, addressing environmental determinants like access to clean water, and empowering community health workers leads to sustainable, measurable outcomes. Policymakers have a critical role to play in building resilient health systems that ensure equitable access to vision care for all.
Read more about our approach to Hospital-Based Community Eye Health.
When I first met Mary*, she told me how she had been blind since 2012. She had started losing her vision when she was very young – when she was a new bride and expecting her first child. Living in a rural area, far from any hospitals, she went to a traditional healer for help but continued to lose her sight. People whispered that she must have been doing witchcraft that backfired on her… asking what else could explain blindness in someone so young. Believing the witchcraft rumours, Mary’s husband left her before the baby was born. Her family abandoned her too. The only person who helped Mary was her niece, who has been supporting her and her child all this time.
When the niece heard that Operation Eyesight was offering free eye exams, she brought Mary to a surgical camp we were hosting. After all her years of alienation, Mary had little confidence in getting her sight restored, but she agreed to a checkup in hopes that it would reduce the eye pain she was experiencing. The team diagnosed her with bilateral cataracts and recommended surgery, which she agreed to.
I went to check on her in hospital shortly after her bandages came off. I was initially disappointed because she kept saying, “No, I can’t see you. I can't see anything.” Worried something had gone wrong with the operation, I called her over to see the doctor, when she finally said, “Actually… I can see you, but I’ve been blind for so long, I thought I was imagining you! I’ve been able to see you the whole time.”
She erupted into laughter, then tears. Her niece joined in.
We escorted her home by bus, and the whole time she was pointing and smiling at things she saw rushing by through the window. She said her greatest excitement was seeing the face of her daughter – now 12 years-old – as soon as she got home.
*name has been changed to protect the patient’s privacy

Candy Siadibbi joined our Zambia team in 2022, first working in the Lusaka area before relocating to Mkushi, in Central Province. She has a bachelor’s degree in psychology and public administration from the University of Zambia. Before joining Operation Eyesight, she worked as a research assistant, freelancing with various nonprofit organizations.
On the day I arrived in Garbatulla, Kenya to begin my work with Operation Eyesight, there was no electricity, so I couldn’t let my colleagues back in Nairobi know that I had made it. The next day, the network came back online, but the incident sums up one of the challenges of working in this area – the difficulty in connecting with people, including many of our community health promoters who live in villages without network coverage.

Many people here in Isiolo County, in Kenya’s arid upper eastern region, are semi-nomadic. They move from place to place in search of pastures for their cows, sheep, goats and camels. Recently, flash floods cut off access to several villages. That’s why the new vision centre we’ve established in Garbatulla – in partnership with Garbatulla Sub-County Hospital – is so important. Now there’s a permanent eye clinic people can visit whenever the roads are open or when herders are back from distant pastures.
When I got here, I stayed at a local mission as I hadn’t found a permanent place to live.
A woman there named Hellen was very kind to me, making sure I got my tea each morning and that I had everything I needed to get settled. When I explained what had brought me to Garbatulla, she said she was struggling with her vision. I encouraged her to come to our clinic, where she was diagnosed with a cataract in her left eye. She was concerned that taking time off would disrupt her duties at the mission, but on the day of her operation she showed up and got it done.
I just had lunch with Hellen recently, and she is doing very well and has made a full recovery. I’m grateful to have helped someone who made me feel so welcome when I first got here

Samson Ngyongesa started working for Operation Eyesight in March 2025. He is the Program Coordinator supporting our Johnson & Johnson–funded Hospital–Based Community Eye Health Project in Garbatulla, Kenya. Samson previously worked for the Asante Africa Foundation, implementing a digital transformation strategy in remote parts of East Africa, and he has a background in economics.

Look at those big, beautiful eyes! This is baby Aarsh, from a small village just outside Moradabad city, in Uttar Pradesh, India. At seven months old, he weighs about seven pounds – what many babies weigh at birth.
Aarsh’s mother, Shabana, was only seven months pregnant when she delivered him prematurely. Little Aarsh had been in an incubator in the neonatal intensive care unit (NICU) at their nearby hospital for 15 days when his parents learned that he needed to have his eyes screened for Retinopathy of Prematurity, or ROP.
ROP is one of the leading causes of vision loss in children, and preterm infants are at high risk of developing this blinding condition. ROP occurs when abnormal blood vessels grow and spread throughout the retina, the tissue that lines the back of the eye. These abnormal blood vessels are fragile and can leak, which can scar the retina and pull it out of position. This causes a retinal detachment and visual impairment.
To save a child’s sight, early detection and treatment of ROP are critical. Unfortunately, many infants go undiagnosed due to the lack of awareness of ROP and the lack of screening services available outside of tertiary-level hospitals. That’s why we are working with partners like C.L. Gupta Eye Institute (CLGEI), located in Moradabad city, to provide remote diagnosis and referral services for at-risk infants and their families. With a case of specialized teleophthalmology equipment and pediatric supplies in hand, optometrists from CLGEI regularly visit 40 NICUs and maternity centres across the Moradabad District, where they capture retinal images of premature infants with assistance from nursing staff who help keep the wriggly babies calm and still.

When Aarsh’s parents first learned their baby could have ROP, they were fearful of the treatment process, and they refused to have Aarsh screened in the NICU. Fortunately, the team at CLGEI are known for their compassion and persistence. After continuous follow-up phone calls and messages from the ROP Coordinator, Aarsh’s parents agreed to bring the little boy, then six weeks old, to CLGEI for screening.
Aarsh’s retinal images revealed that he had ROP in both eyes and required urgent treatment to prevent blindness. First, his eyes would be injected with a drug that inhibits abnormal blood vessel growth, then, at a later appointment, he would receive laser treatment.

Shabana couldn’t help but get emotional she when she heard Aarsh’s little cries from the next room as the doctor did the injections. She knew that timely treatment was necessary to save her son’s sight, but still the tears streamed down her face. Her little one wasn’t even two months old, and he’d already been through so much.
Following the injections, Aarsh’s eyes were covered with bandages, and they were sent home that same day with eye drops and a list of post-procedure instructions. No doubt, the experience was a lot for Aarsh’s parents to take in, worrying about their newborn baby who required special care while also tending to their other children; but they took comfort in knowing that the pediatric staff at CLGEI were available to help them every step of the way.

Later that week, Aarsh received laser treatment. The procedure, which is done with local anesthetic, uses a beam of light to create scar tissue on the outer edges of the baby’s retina, which prevents abnormal blood vessels from forming.
Aarsh’s family went for several follow-up visits. His parents were diligent about making and keeping their appointments, even though it meant that his father, Ajmat, had to close his shop so they could travel to the hospital, which meant a loss of income. They were thankful that Aarsh’s treatment was provided free of charge. They were also grateful to the CLGEI staff who checked in with them and sent them reminders.

Today, Aarsh is doing great, and his vision is good. His mother, who is also happy and in good health, says that Aarsh even watches cartoons on the television like his big brother and sister.
“Little Aarsh's journey is a testament to the transformative power of our ROP screening program. Through the dedication of our team and the support of generous donors, we're not just preventing blindness; we're nurturing futures," says Lokesh Chauhan, Deputy General Manager at CLGEI.
“Aarsh's bright eyes now reflect a world of possibilities, and his story motivates us to continue our mission of bringing vision and hope to every child in need."
Aarsh will require lifelong follow-up visits. Doctors have stressed to his parents the importance of regular eye exams, as infants with ROP are at higher risk for developing other eye problems later in life, such as myopia (nearsightedness), strabismus (crossed eyes), amblyopia (lazy eye) and glaucoma. In many cases, these eye problems can be treated or controlled.

Thanks to the generosity of our donors, the diligence of Aarsh’s parents, and the expertise of the staff at CLGEI, little Aarsh has a big future ahead of him.
Please donate today to help more infants like Aarsh.
Dr. Ashi Khurana, Vice-Chairman, C.L. Gupta Eye Institute is a cornea specialist and manages the Retinopathy of Prematurity Eradication Project. The project screens premature infants in Moradabad and five surrounding districts for Retinopathy of Prematurity (ROP), which can cause irreversible blindness if left untreated.
World Prematurity Day: Dr. Ashi Khurana, Vice-Chairman, C.L. Gupta Eye Institute on preventing blindness in premature babies
An eye condition that is all but invisible to parents, pediatricians and the community can silently rob premature and low-weight infants of their sight. The condition must be treated early or the infant can go blind, not as a baby, but years later as a child. The condition is called Retinopathy of Prematurity (ROP), and in 2016, it became all too visible to eye doctors at C. L. Gupta Eye Institute.
Dr. Khurana remembers a doctor coming to her and being “very concerned as they found that a lot of children were coming in and had gone blind due to ROP.” It was a major problem that no other organization was addressing. ROP can be treated but it requires screening, diagnosis and urgent treatment that can include injections and laser eye surgery.

However, there was no widespread public health initiative to address ROP. Dr. Khurana and her team saw the shadow that blindness from ROP caused on children, their families, the health care system and society. Though a small number of babies develop ROP and lose their sight, “there is a huge impact on the life of that child and their family because someone, often the mother, becomes the caregiver.” There is a direct impact on the mental, physical and financial resources in a family, she says. Later treatment is also often complex, intensive and has poor outcomes. “It is very frustrating as a doctor,” says Dr. Khurana, “when there is not much you can do for a condition that could have been prevented.”
Conditions impacting premature infants, such as ROP, are on the rise

Premature births are a global issue. The World Health Organization data from 2020 estimates that 13.4 million babies, or one in 10, were born premature.
India has the highest prevalence of premature births in the world. Data from the Lancet found that three million premature babies were born in India in 2020.
The emergence of local NICUs has greatly increased the survival rate of premature infants. This has led to a shift from survival to quality of life by addressing the complications of prematurity. “ROP is a modern disease as more babies survive due to high quality NICUs,” Dr. Khurana says.
Conditions of Premature Infants on the Rise
To address the growing need and fill the gap in service, Dr. Khurana and her team launched an ROP screening program in Moradabad, Uttar Pradesh, India. Initially it was a pilot and then it expanded to include a partnership with Operation Eyesight Universal and was called the Retinopathy of Prematurity Eradication Project.

On a mission to raise awareness and start screening for ROP
At that time, Dr. Khurana remembers that C. L. Gupta Eye Institute was not getting a lot of referrals from pediatricians to screen the eyes of premature infants for ROP. She knew that they needed to start an awareness campaign to educate doctors and pediatricians about ROP and the need to screen. “It should just happen, like a vaccine,” Dr. Khurana says.
The team started knocking on doors and going into NICUs to talk to not only doctors but also NICU managers and nurses, who are often the ones responsible for requesting ROP screenings.
Screening requires specialists and equipment often found in an eye hospital. As premature infants cannot travel and spend their first few weeks in emerging NICUs, the screening needs to take place there. However, many of the infants are fighting for their lives. “They have a lot of complications and there is a lot of priorities for doctors and stress for families,” Dr. Khurana says. “And then with all that, this issue of blindness comes up.”
There are also a limited number of eye doctors, and it can be challenging for them to travel to multiple NICUs to screen premature infants “who may or may not have an eye problem.”
An ambitious screening goal
The initial goal was to screen 500 children “which was huge,” Dr, Khurana says. To achieve this they sent optometrists to screen premature infants for ROP regularly at 40 local NICUs. Infants with ROP were referred to C. L. Gupta Eye Institute for urgent treatment.
In the first phase, the team screened 464 premature infants and saved 50 children from blindness. “It has been very satisfying for our doctors,” Dr. Khurana says.
In addition to raising awareness among medical staff, Dr. Khurana’s team started to educate the community as well. Not all parents are able to understand why screening and treatment are needed. There can be literacy and poverty issues that need to be addressed and at times, parents may deny treatment. Gender can be a factor as can birth order, if there are many children in the family.
People who can pay do, those who can pay part of the cost contribute what they can and those who cannot pay are supported by Operation Eyesight Universal. In this way, “everyone receives care and treatment.”
The second phase of the project launched on July 16, 2024, expanding beyond Moradabad to Sambhal, Bijnor, Amroha, Rampur and Baduan. Reaching these semi-urban areas was possible due to a mobile van with the required equipment, made possible through the Rotary Foundation, for onsite screening and treatment in rural and underserved areas, a tele-ophthalmology platform that allows experts to provide remote consultations, diagnoses, and treatment recommendations, an expanded network of neo-natal intensive care units in the five new regions and continued medical education to raise awareness of ROP, capacity and skills of NICU staff in the additional districts.
In December 2024, the Retinopathy of Prematurity Eradication Project ends. Services will be maintained with C. L. Gupta Eye Institute, a non-profit, covering costs for those who cannot pay, and working with NICUs.
ROP is a modern disease that requires resources

ROP is being studied and the ROP Society of India is looking at the impact of the condition on the country. As more NICUs emerge and more premature infants survive, ROP is appearing more frequently.
Now, Dr. Khurana and her team are working to raise awareness of ROP in the community, among parents and with medical professionals. What is needed is more resources, public health support and training for doctors.
For now, her team is small but dedicated. “It is satisfying for us to make a difference in the lives of these children and families,” she says.
For the premature infants and their families in and around Moradabad, there is hope of a bright future.
See how this this project works in the video Born Too Soon: Retinopathy of Prematurity Project, Moradabad, India.
Read about how this project transformed the life of Baby Aarsh and his family.
Imagine preparing a meal for family and friends, and nobody eats it because they don’t trust your cooking skills due to your failing eyesight.
Or picture yourself shopping at the local marketplace and wondering if you’re being shortchanged by the vendor because you can’t see the numbers on the coins.
That’s what Sharda, who lives in a village in Uttar Pradesh, India, experienced during her 35 years of near-blindness.
Until recently, Sharda had never seen her grandchildren’s faces.
The grandmother started losing her eyesight after being bitten by a snake – an injury that affected both eyes. During a hospital visit, a health worker told her that they couldn’t do anything to help her, even though Sharda was in a position to pay for eye health services. She travelled all the way to Punjab, where her sister lives, to see if she could get help there, but once again, she was turned away without treatment.
One day, Sharda met a community health volunteer who was going from house to house as part of our project with the C. L. Gupta Eye Institute (CLGEI) in nearby Moradabad. The volunteer quickly assessed Sharda’s eyes and concluded that she had cataracts, and gave her a referral to CLGEI, where she got a formal diagnosis and an appointment for surgery.
After getting both cataracts removed, Sharda was amazed at the dramatic recovery of her vision. She could finally see her grandchildren clearly.
Today, Sharda is back to cooking and shopping, and once again feels loved and valued by her family. With a new lease on life, she tells everyone she knows about the CLGEI vision centre and how staff there helped her regain her sight.
This now-tireless eye health ambassador has her sights set on her next project: her husband. Sharda says she’s taking him to the hospital soon to get his cataracts removed as well.
You too can be an eye health ambassador – please share our website with others or make a donation.
Holding an awl in one hand, and a man’s leather shoe in the other, Abraham in Kenya demonstrates how he pierces a hole in the leather before stitching it up to make a repair. It’s part of his job as a cobbler that, for months, he was unable to do.
A couple years ago, Abraham started having trouble with his vision. His work suffered as he had more and more difficulty focusing his eyes on the tiny stitches and delicate work of shoe repair. He began pricking himself repeatedly with the needles, and eventually, he couldn’t get the needles threaded at all. Finally, he had to shutter his business.
At age 65, Abraham’s six children are now grown up, but his income was essential to supporting his grandkids. Without being able to repair shoes, he had to rely on his wife’s earnings as a farmer to get by.
The loss of income wasn’t the only financial difficulty exacerbated by his vision loss. Because he couldn’t see well enough to punch in his PIN on his phone, Abraham started giving the number to shop attendants while making purchases. Eventually he realized that some of them were stealing from him and transferring additional money to themselves before handing the phone back over.
Abraham went to a nearby clinic for help with his vision. He received a prescription for eyedrops, but his condition continued to worsen despite regularly using the drops.
One day, Abraham met one of our community health volunteers, who was going house to house doing eye health screenings. The volunteer gave Abraham a referral to the eye unit at our partner facility, the Iten County Referral Hospital, where he was diagnosed with cataracts in both eyes.

Just weeks later, Abraham went back to the Iten Eye Unit. The surgeries on both eyes were a success, and when our staff caught up with him, they were impressed with how quickly he had bounced back. He has started repairing shoes again and is happy to be taking care of his family with the income. He has also become an eye health ambassador, telling his neighbours about the Iten Eye Unit and how eye surgery transformed his life.
Please consider making a donation to help more people like Abraham get back to work!
Story written with files from Caroline Ikumu.
Herding cows is such a fundamental part of Maasai culture that it is common to hear people in that community greeting each other with, “I hope your cattle are well!”
So, when 70-year-old Parmuat, a Maasai herder in Kajiado County, Kenya, thought he might have to sell off his cows, he was devastated.
Several years ago, Parmuat looked outside his home and couldn’t see his cows anywhere. When he found them, he realized they had been right in front of him all along, on a hill near the house. He hadn’t been able to see them because of his increasingly blurry eyesight.

As his vision got worse, Parmuat found it harder and harder to care for his herd. He didn’t know how else to make an income, and he worried that he and his wife would become a burden to their 12 children, now grown up and raising families of their own.
Parmuat’s luck changed when a community health assistant, whom we’d trained in primary eye care, knocked on his door during a door-to-door eye screening and diagnosed him with cataracts.

Just a few weeks later, Parmuat learned he would be among the first patients to get cataract surgery at the new eye unit at the Kajiado County Referral Hospital.
After surgery, when a nurse removed the gauze from his eyes, Parmuat marveled at his restored vision. “Everything was clear again,” he says, “as if the sun suddenly came up.”
Now back at home with his wife, Parmuat says that he doesn’t need to sell any cows. In fact, he adds with a twinkle, he’s thinking about buying a couple more.
With files from Patrick Wainaina
Reaching the remote village of Kachikata, in India’s northeastern Assam state, is no small task. The journey from Jorhat, the nearest city, begins by jeep on rough roads leading down to the Brahmaputra River. From there, travellers climb onto a tiny ferry, big enough only for a handful of passengers, that takes them to Majuli Island. After the boat arrives on the island’s shores, the journey continues by motorcycle, tractor or bullock cart to reach the village.
This makes medical care difficult to access, especially for seniors like Gadami.
For six years, the grandmother lived with cataracts in both eyes. As her vision worsened, she became reliant on family members to help with even simple tasks.
“There was no doctor, no eye camp, nothing,” says our Program Manager Tapobrat Bhuyan, describing the community when he first visited it in 2021.

When community health volunteer, Dipen, met Gadami during a door-to-door screening, he referred her to a nearby eye camp. There, she was diagnosed with bilateral cataracts, and agreed to make the long journey to Jorhat, where she received sight-restoring surgery at our partner hospital, Chandraprabha Eye Hospital, free of charge.
Gadami’s granddaughter, Junu, was by her side to comfort her during the hospital stay and share in her joy when the bandages came off.
Back in Kachikata, Gadami’s world has opened up. With her independence restored, she can once again walk around the village, visit friends and fully enjoy her time with her grandchildren.
Watch a video about our work on Majuli Island!

